
In this article, let's discuss ‘intralesional curettage’.
As opposed to 'wide resection', 'intralesional curettage' is not the removal of the entire bone and the 'whole' tumor but the removal of the tumor piece by piece. The following figures distinguish the two surgical methods:
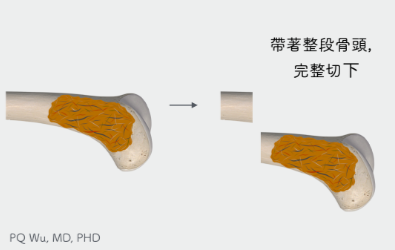
Wide Resection .
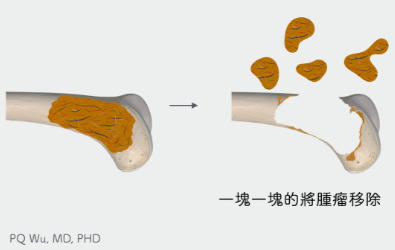
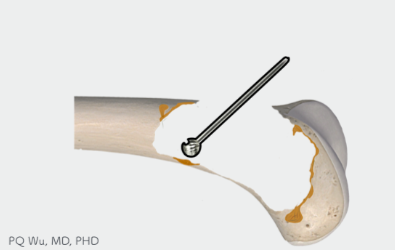
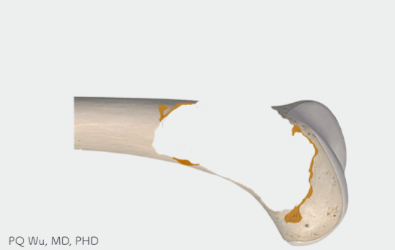
Intralesional Curettage
As shown in the figures above, wide resection removes the entire bone and the soft tissues near the bones, including muscles, ligaments, tendons, and even cartilage, etc. Hence, the patients will need more time to recover after surgery. Relative to wide resection, intralesional curettage will need only a smaller wound. With an opening on the bone at the tumor, the tumor can be removed. Therefore, it destroys the bones and surrounding soft tissues less during surgery, and the patients will recover faster with better limb functionalities!
However, in contrast, since intralesional curettage removes tumor piece by piece, it may not remove the tumor completely during surgery. As a result, the chance of tumor recurrence is higher than that of wide resection.
Wide resection
- Greater damage
- Long surgery time and more difficult
- Slower recovery and poor function
- Tumors are more likely to be completely removed and have a lower chance of recurrence
Intralesional curattage
- Lesser damage
- Short surgery time and easier
- Quicker recovery and better function
- Tumors may not be completely removed, and the chance of recurrence is higher
Based on the characteristics mentioned above, the main indications for intralesional curettage include:
Benign bone tumors
In general, benign bone tumors have a lower recurrence rate. Hence, to retain better functionality, intralesional curettage is the most used method.
Benign soft tissue tumors
Intralesional curettage can be applied. However, unless the tumor size is too large, we recommend removing the whole tumor for general benign bone tumors.
Cancer combined with multiple bone metastasis
When other cancers combine with multiple bone metastasis, the treatment objectives are 'reduce pain', 'avoid pathological fractures', and 'recover rapidly'. Hence, intralesional curettage is used.
Malignant bone tumors that invade vital organs
For a small number of primary malignant bone tumors, such as osteosarcoma, if they grow in the pelvis, spine, or other positions and invade or adhere to the vital organs, we would conduct intralesional curettage since wide resection would influence patient life
Low-grade malignant bone tumors
For ‘lower’ grade malignant bone tumors such as low-grade osteochondroma, we can use intralesional curettage with adjuvant therapy to remove the tumor and retain better life functionalities.

Step 1: Intralesional curettage for bone tumor at the distal femur
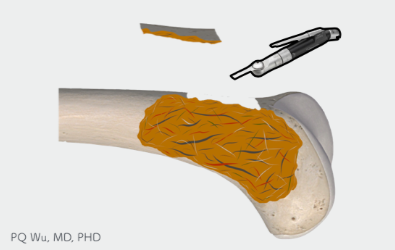
Step 2: First, use a saw blade to create an opening at the tumor site
Step 3: Use different sizes and angles of curettes to remove the tumor piece by piece

Step 4: Visual inspection to confirm no visible tumor repeatedly.
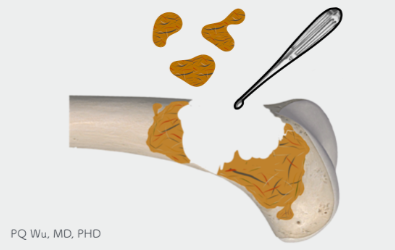
Step 5: Finally, use a high-speed burr to polish the bone cavit
Step 6: Almost all the tumors can be removed, yet there’s still a chance to have residual tumors.
The following figure shows the use of a curette during surgery, as mentioned in Figure 3 above. In this step, it takes a lot of time to carefully clean up the tumor to reduce recurrence. Generally, after this step, about 95 percent of tumors should have been removed.

Curette for surgery
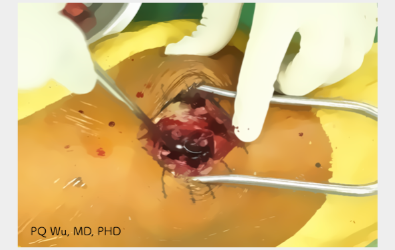
The process of surgically scraping a tumor
The figures below show the use of high-speed burr during surgery, as mentioned in Figure 5 above. A high-speed burr can remove the remaining tumor attached to the bone and the surrounding part of the normal bone cleaner. Generally, after this step, almost 99% of tumors should have been removed. In this step, care must be taken, as high-speed burr can easily drill the bones empty, and if used in the same area for too long, it can cause excessive bone defects and even pathological fractures.

High-speed burr used in surgery
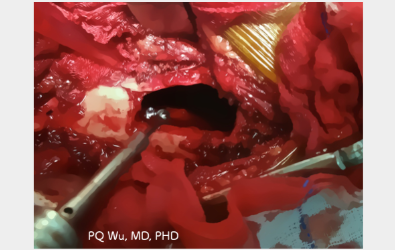
The surgical process using a high-speed burr to remove tumor
Since the recurrence rate is low for the following bone tumors, it’s sufficient to use the two aforementioned surgical curettage and high-speed burr processes.
- Osteochondroma
- Fibrous Dysplasia
- Simple Bone Cyst
- Osteoid Osteoma
- Enchondroma
However, for other bone tumors below, because the recurrence rate is higher and the local damage is strong, the use of the two aforementioned surgical curettage and high-speed burr processes would still bring a fairly high chance of recurrence.
- Giant Cell Tumor
- Aneurysmal Bone Cyst
- Chondroblastoma
- Osteoblastoma
- Eosinophilic Granuloma
- Enchondroma
- Bone Metastasis
- Low-grade Bone Sarcoma
Hence, for the tumors mentioned above, we must also perform adjuvant therapy, including the use of phenol, alcohol, and liquid nitrogen to greatly reduce the tumor recurrence.
It is not the end of the surgery after tumor removal. Although the tumor has been removed, the hole caused by the tumor before surgery remains. So, we also need a second surgery step- 'bone transplantation after intralesional curettage'. We have to use different 'materials' to fill in the bone defects to avoid subsequent complications such as fractures. The following links provide more information on bone transplantation.
Regular post-surgical outpatient tracking is required. The doctor will determine how much force you can step on and when you can be free from crutches based on how well your bones recover. After full recovery, there's a chance of tumor recurrence, and regular X-ray or MRI checks will still be needed to detect and treat problems early.