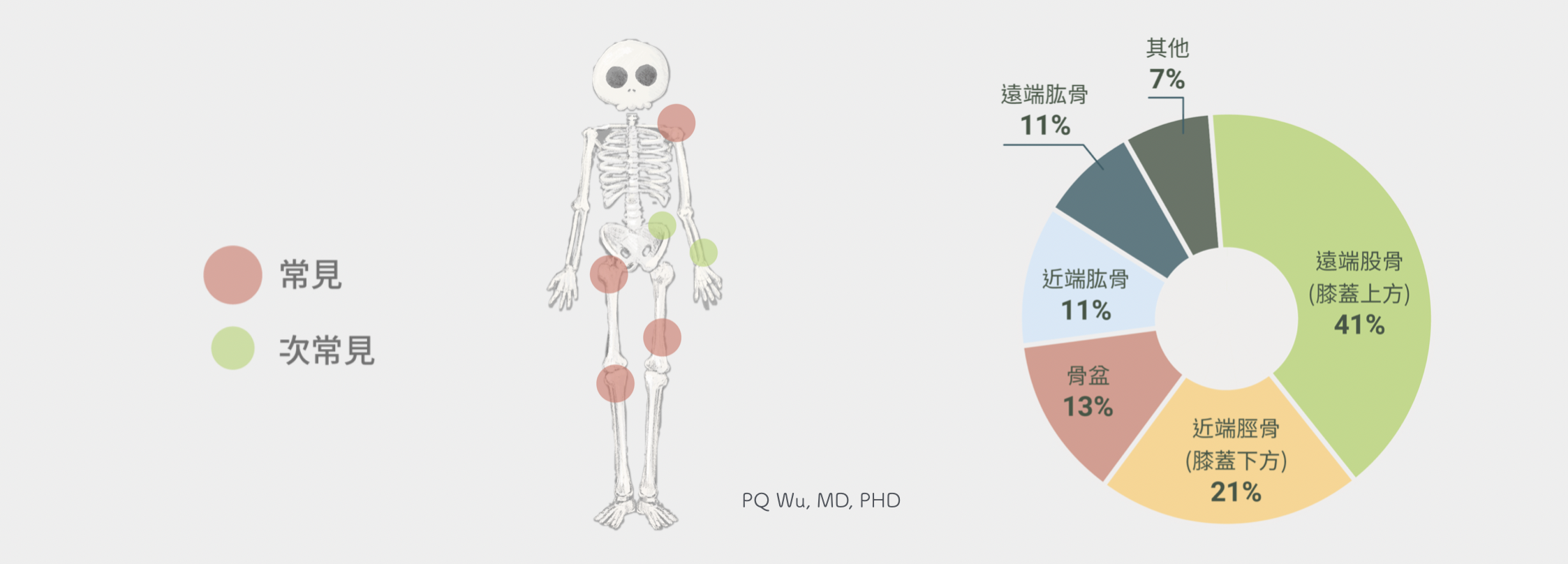
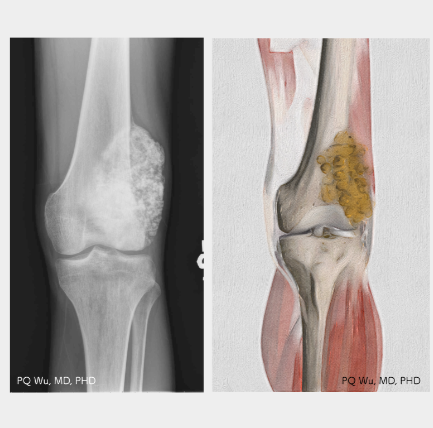
Osteosarcoma can occur on any bone. The most commonly occurring positions are near the knee, including the upper knee (distal femur, the most common) and the lower knee (proximal tibia, second-most). These locations are also the essential joints affecting our daily lives and exercise. Other locations are shoulders (proximal humerus, third-most) and near the hips (proximal femur). Shoulders and hips are also critical joints. Therefore, often after osteosarcoma surgery, patients are always affected in their life function. The degree of impact is highly related to the pre-operative damages from the tumor, the orthopedic surgeon's capability to reconstruct limbs, and patients' postoperative perseverance.
In general, surgery for osteosarcoma here is relatively easy (but not absolute), and the postoperative functional recovery is better.
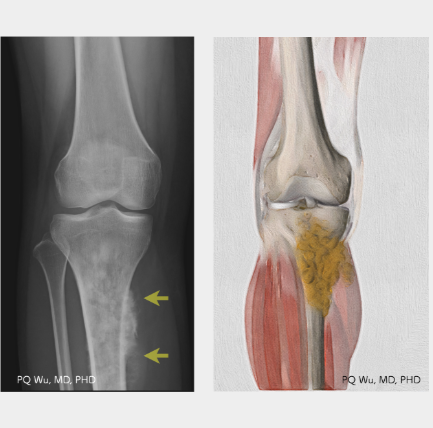
The most difficult part in the proximal tibia surgery is to deal with the patella tendon and reconstruct the extensor mechanism of the knee. If the tumor is severely invasive, the surgical reconstruction is poor, or the patient's perseverance is insufficient, the strength of the knee extensor after surgery will be much worse. In addition, a peroneal nerve controlling ankle dorsiflextion grows near the distal tibia. Therefore, in order to achieve a safe surgical range during surgery, it is sometimes necessary to sacrifice this nerve. In addition, because the skin here is thin and muscle is insufficient to cover the bone, the infection rate after surgery is higher. Often, a gastrocnemius flap transplant is required to increase the coverage of soft tissue.
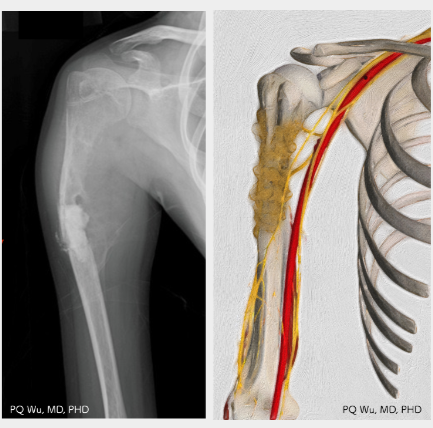
Proximal humerus surgery is known difficult as it contains many bleeding points. Many small blood vessels align at this location, and a tourniquet cannot be applied on the shoulder; hence, the visibility for operation is always influenced. Also, this location is the important place of muscle orgin and attachment for quite a few upper limbs, such as rotator cuff, pectoralis major, latissmus dorsi, deltoid, biceps brachii and triceps. Therefore, intense rehabilitation is required after surgery, otherwise the function of shoulder lifting will be significantly limited. In addition, if the tumor invades larger range outside the bone, the surgery often demages the radial nerve, resulting in the inability to raise the wrist (drop wrist).
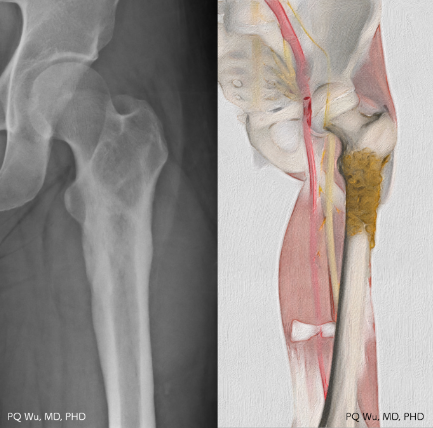
The proximal femur is the critical place of muscle origin and attachement for numbers of lower limbs, such as gluteus medius, gluteus minimum, three of the quadriceps (vastus medialis, vastus intermedius, vastus lateralis), etc. Therefore, intense rehabilitation is required after surgery, otherwise the function of walking will be significantly limited. In addition, if the tumor invades larger range outside the bone, the surgery often demages the femoral nerve, resulting in the inability to straighten the knee. Moreover, if the tumor invades the back, the surgery may demage the sciatic nerve, leading a drop foot.
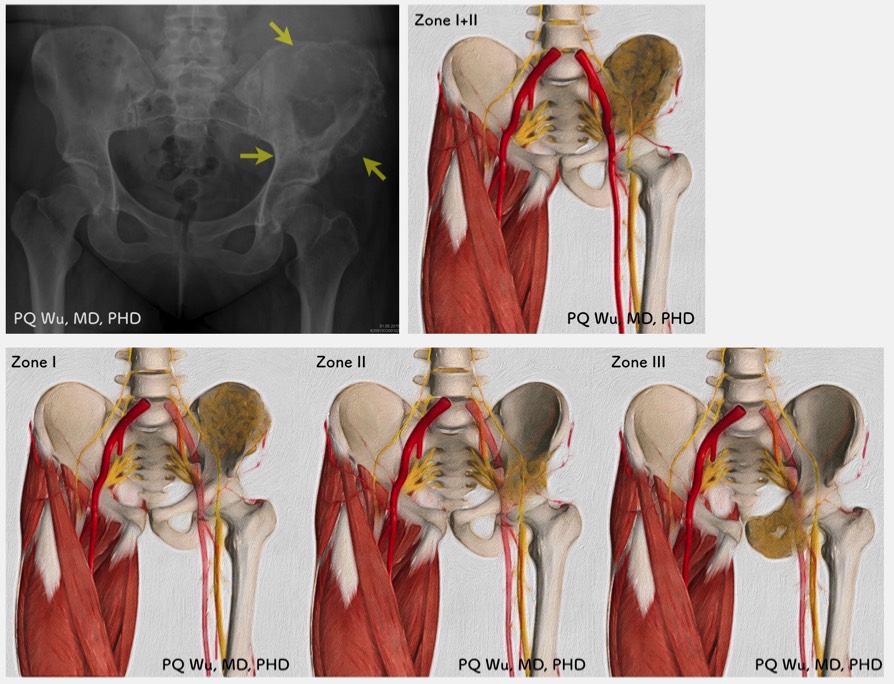
It's unlikely (approx. 6%) to have tumors occur near the axial skeleton, including the pelvis, spine, and shoulder blades. The osteosarcoma at the pelvic cavity is hard to diagnose because it has low palpability and the symptoms are often similar to the spinal disc herniation. Hence,when a patient is diagnosed with a malignant bone tumor, the tumor is often quite large and often with lung metastasis. Moreover, since it is very close to important nerves such as sciatic nerve and femoral nerve, and important blood vessels such as internal iliac artery and eternal iliac artery, surgical excision and limb reconstruction are 'quite difficult' and 'quite risky'.
(Dr. Wu: Generally, if we know that we will carry out pelvic tumor surgery the next day, we will ensure full sleeps and sufficient breakfast or lunch the day before. We will also drink two glasses of concentrated black coffee before the surgery!)