
According to the pathological pattern, osteosarcoma can be divided into several subtypes. Common subtypes include osteoblastic, chondroblastic, fibroblastic, and telangiectatic; Other rare ones include small round cell, giant cell-like, chondroblastoma-like and mixed type. The influences of subtypes on prognosis are still not conclusive among various cancer research centers. Generally, chondroblastic osteosarcoma is considered to have a poor response to chemotherapy, but the influence of various subtypes on the prognosis is small. However, not all osteosarcomas are seriously malignant tumors. Less than 25% of them have low-grade malignancies. These tumors grow mainly outside the bone without invading the bone marrow, and the prognosis is fairly good without the required chemotherapy. We will discuss more the low-grade malignant osteosarcoma in another section.

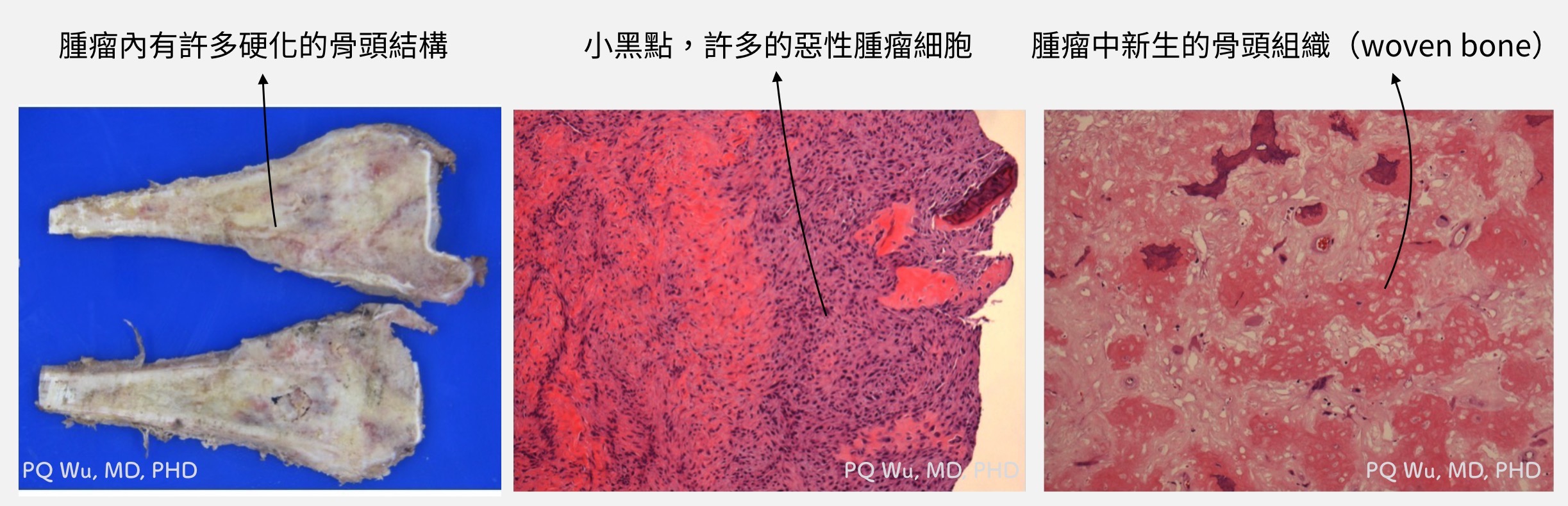
Most of the osteosarcoma observed clinically are osteoblastic osteosarcomas. Many new bones can be seen in the pre-operative X-ray image and the tumors during operation. These newborn bones are even harder than normal ones. Overall, osteoblastic osteosarcoma has a solider structure, and it's thus relatively safer and simpler for surgery.
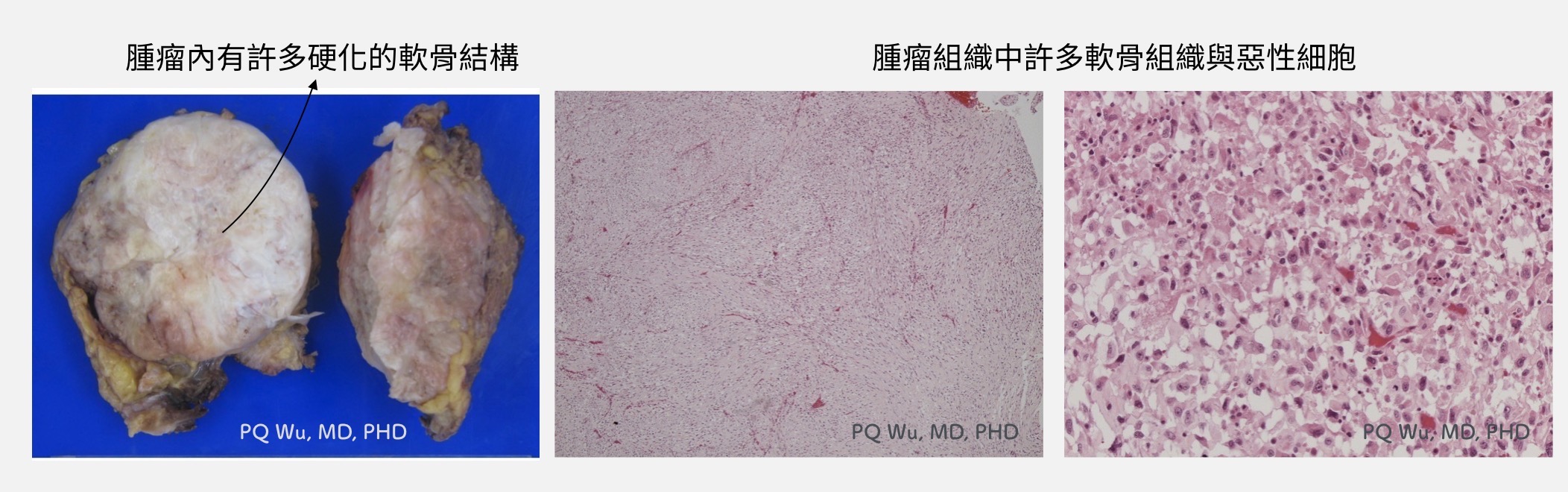
Chondroblastic osteosarcoma is about 25% clinically. Pathologically, it is sometimes not easy to distinguish from malignant chondrosarcoma. Often, only limited information could be obtained in biopsy examination. However, distinguishing between chondroblastic osteosarcoma and chondrosarcoma is sometimes important since it is related to the choice of conducting chemotherapy or the option of drugs for treatment.
Fortunately, two important studies were published in 2011 and 2013 (Note 1). In 2011, a pathologist at Royal National Orthopaedic Hospital in the UK found the somatic mutation of isocitrate dehydrogenase 1 (IDH1) and IDH2 occurs in the tumors developed from cartilage, such as chondrosarcoma. In 2013, IDH1 and IDH2 were used by Massachusetts General Hospital in the US to distinguish chondroblastic osteosarcoma with chondrosarcoma. Other than the cartilage originated chondrosarcoma, chondroblastic osteosarcoma is originated from mesenchymal cells, and it won't have IDH1 and IDH2 expression. Therefore, the IDH gene expression provides considerable help in distinguishing the two types of tumors. (Dr. Wu: Unfortunately, such gene testing is currently not reimbursed by the National Health Insurance in Taiwan. The test will charge out-of-pocket, and only a small number of hospitals have the test capability).
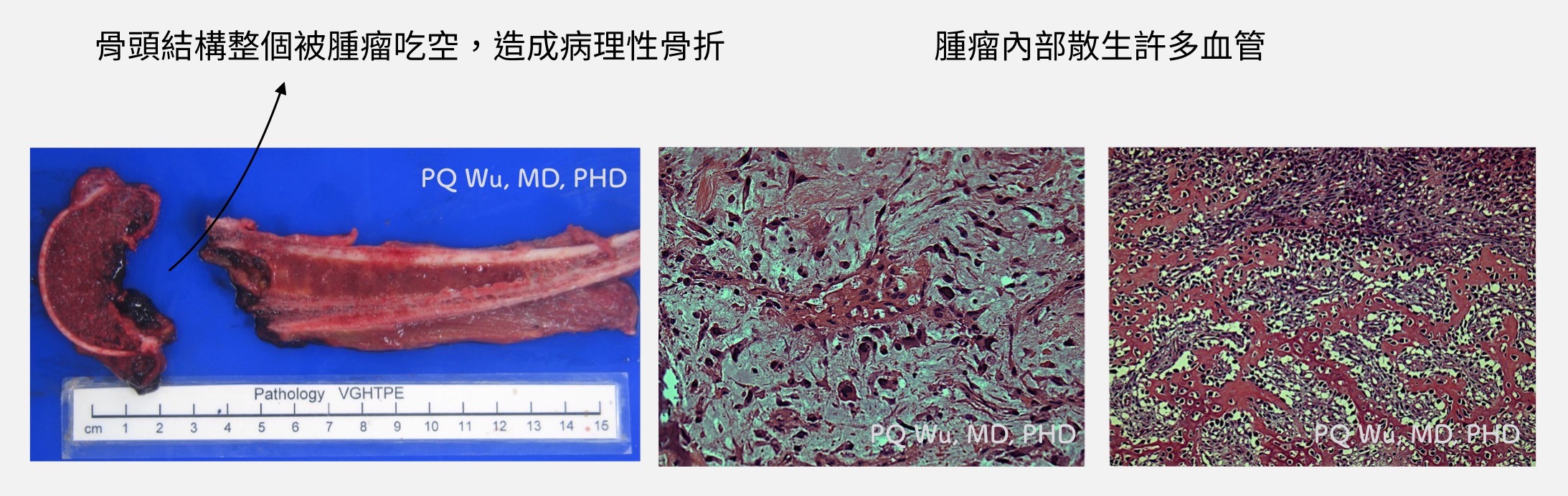
Telangiectatic osteosarcoma is about 2%-12% clinically. Clinically, it often causes more severe bone defects. According to the study published in the journal cancer in 2007 by the team at St. Jude Children's Research Hospital, 43% of the cases would have pathological fractures resulted from severe bone defects. It would thus easily lead to local recurrence and metastasis once pathological fractures occurred. Radiologically and pathologically, it has a similar expression of aneurysmal bone cyst that occurs in benign tumors. As a result, telangiectatic osteosarcoma is often mistakenly treated as benign tumors and brings serious clinical effects (Note 2). Telangiectatic osteosarcoma is thus considered a nightmare for physicians specialized in osteosarcoma
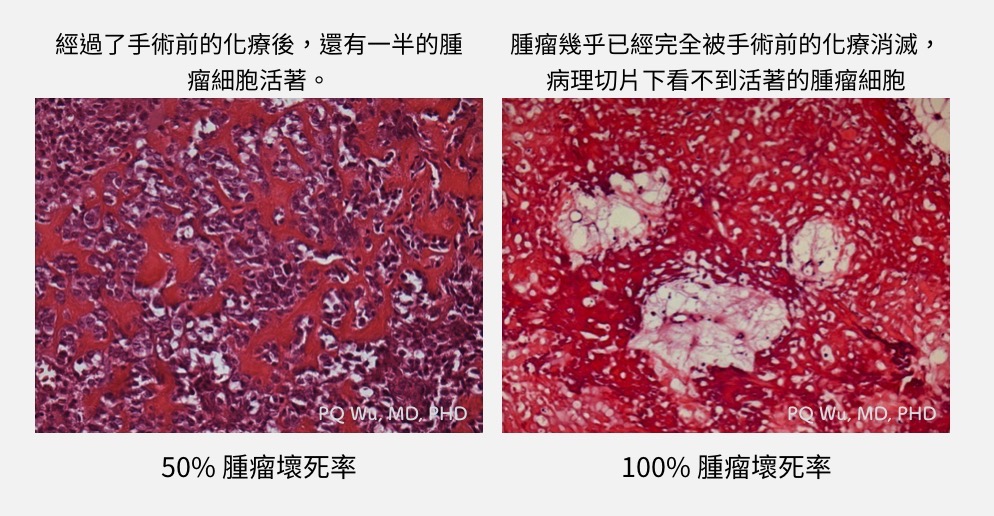
Another more important pathological examination is to determine the post-neoadjuvant chemotherapy tumor necrosis rate in addition to morphological observation for osteosarcoma. Tumor necrosis rate is considered the most important indicator that affects patient prognosis. The higher the necrosis rate, the better the efficacy of neoadjuvant chemotherapy two months before surgery. The current international consensus is that if the tumor necrosis rate is greater than 90% (some think 99%), a better prognosis is anticipated. Meanwhile, we also determine the drug dose based on the tumor necrosis rate for postoperative adjuvant chemotherapy.
note1 :
IDH1 and IDH2 mutations are frequent events in central chondrosarcoma and central and periosteal chondromas but not in other mesenchymal tumours. 2011.
Molecular Distinction of Chondrosarcoma From Chondroblastic Osteosarcoma Through IDH1/2 Mutations. Am J Surg Pathol.
note2 :
Telangiectatic osteosarcoma: a review of literature. OTT. May 2013:593.
Telangiectatic osteosarcoma: The St. Jude Children“s Research Hospital”s experience. Cancer. 2007;109(8):1627-1637.