
As mentioned earlier, "wide resection" is traditionally defined as removing the tumor from the edge of the tumor and two to three centimeters of normal tissues. There is no firm definition of how many centimeters of normal tissues should be removed. Articles decades ago recommended that the edge should be at least 3 centimeters or more. Still, because of the great preoperative chemotherapy and accurate imaging technologies, it is generally considered that one to three centimeters of the safe range is sufficient.
Therefore, this ‘one centimeter safe range’ allows us orthopedic surgeons to develop new tumor removal methods under special tumor conditions. The methods include:
1. Hemicortical resection
2. Hemicondylar resection, which is derived from hemicortical resection and retains one side of the cartilage
3. Epiphyseal preservation
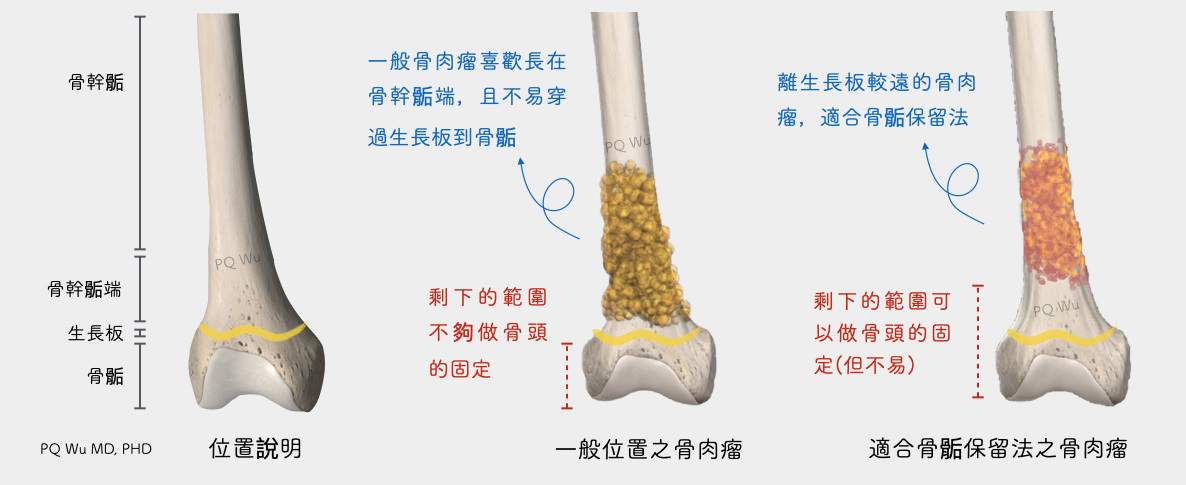
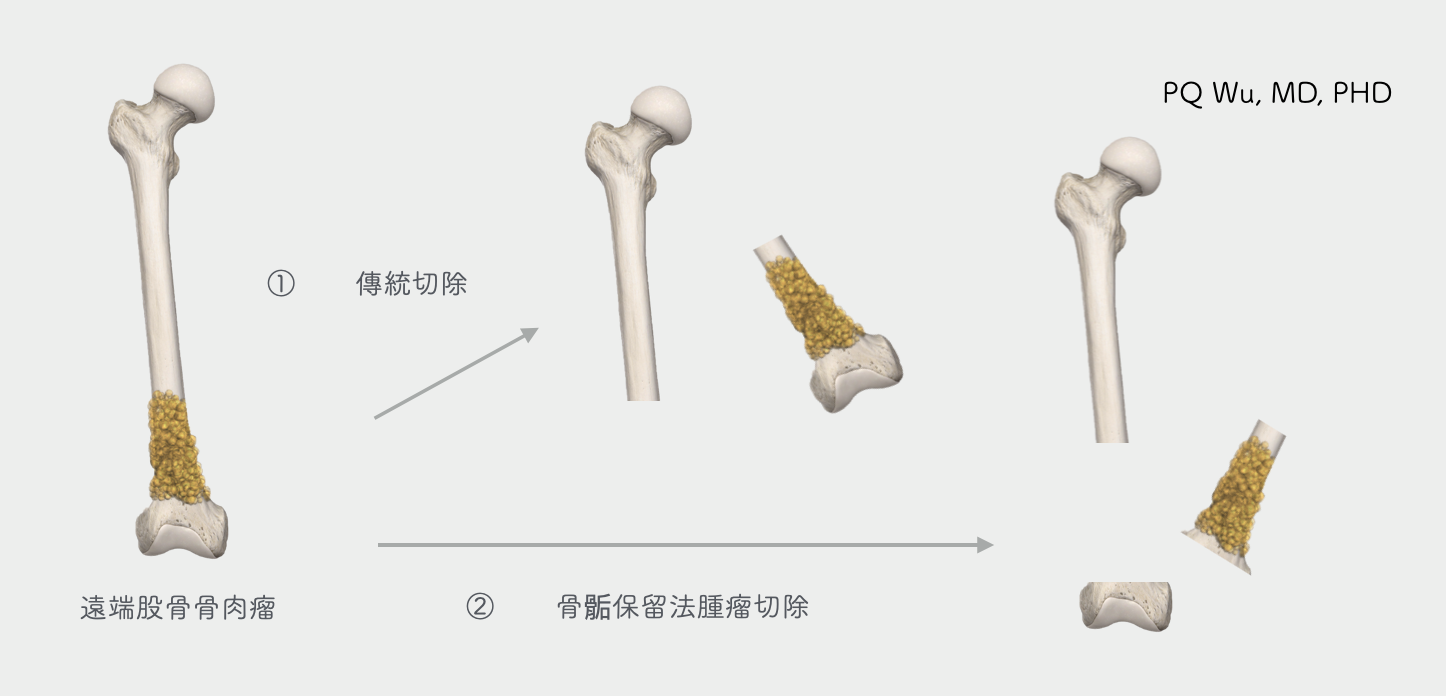
Epiphyseal preservation applies to a small portion of tumors (less than 20%) found relatively far from joints, which are located near metaphysis or even diaphysis. We use epiphyseal preservation to retain the patient’s original joints. The farther away the tumor is from the joints, the more length of bone we have left in the body after tumor resection. When reconstructing the bones, physicians are more likely to re-fix the inactivated, clean bone back into the body. Conversely, if the tumor grows closer to the joint, less after-surgery bone length left in the body provides less support to the inactivate, clean bone, failing reconstruction. The following figures depict the scenario more clearly.

The advantage of epiphyseal preservation over traditional surgery is that we retain the joint cartilage without replacing the artificial joints, and do not worry about future artificial joint loosening. In addition, complete retaining of knee ligament- the anterior cruciate ligament, posterior cruciate ligament, medial collateral ligament, and lateral collateral ligament- facilitates better post-surgical function recovery (of course, the most important thing is the patient's rehabilitation exercise).
However, the surgery also has some limitations and disadvantages:
1. When the remaining normal bones in the body are less after tumor resection, bone fixation for reconstruction is not easy. At this point, we may need to use the 'Locking plate system' with out-of-pocket cost or plaster to fix it for a few weeks.
2. The quality of the MRI image before surgery must be quite good and show the correct range of tumor invasion.
3. Surgeons must have considerably abundant experiences with bone tumor surgery.
4. Cartilage degeneration may happen years after surgery, but generally, it won’t lead to critical clinical symptoms.
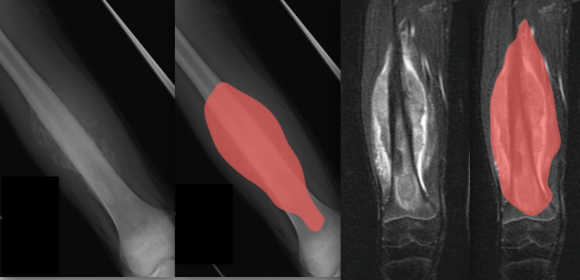
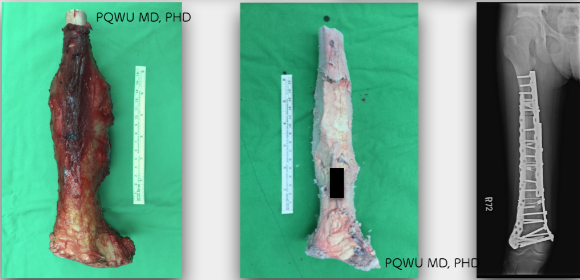
Case 1: A 22-year-old woman with malignant osteosarcoma above the knee bone. The tumor was removed by epiphyseal preservation approach.
The preoperative X-ray showed that the tumor invasion was far from the articular surface so that the epiphysis and joint could be preserved. MRI also reveals a clear tumor range.
By carefully selecting tumors, Epiphyseal preservation is a fairly good method. Patients can retain their normal joint structure after surgery!